At a recent school board meeting in Los Angeles, the budget director put up a slide with a dire warning. Los Angeles Unified, the second-largest school district in the country, is on pace to spend more than half of its annual budget on retirement and health-care costs by the year 2031. By then, it is projected to spend 22.4 percent of its budget on pensions and 28.4 on health-care benefits for current and former workers.
At a recent school board meeting in Los Angeles, the budget director put up a slide with a dire warning. Los Angeles Unified, the second-largest school district in the country, is on pace to spend more than half of its annual budget on retirement and health-care costs by the year 2031. By then, it is projected to spend 22.4 percent of its budget on pensions and 28.4 on health-care benefits for current and former workers.
The cost of health care is rising rapidly in all parts of our economy, but the pressures in the public sector, and particularly in public education, are different. Like many school districts, where salaries are low compared to private-sector peers, Los Angeles Unified School District (LAUSD) has chosen to compensate by providing its teachers with generous health benefits. In fact, the district extends medical, dental, and vision coverage not just to current employees but also to retirees and their spouses, who do not pay premiums or deductibles and yet qualify for full benefits for life. So LAUSD’s projected health-care spending includes 38,000 former workers and spouses, each of whom is estimated to cost up to $291,000 during their retirement years.
LAUSD is an outlier in terms of how generous those benefits are, and the district has begun to roll back who is eligible to receive them over the past decade. But this illustrates a little-understood way public employees like teachers are increasingly diverging from their private-sector peers: they are much more likely to receive health-care benefits after they leave their jobs. Nationwide, the estimated liability for post-retirement health-care benefits for public employees is $692 billion.
Teacher retiree health care is perhaps the ultimate arcane issue in the education sector. There are no funders investing in solutions to this issue, there are few reliable sources of data, and until recently, states and districts did not even calculate how much they had promised in future benefits, let alone start saving to pay for those promises. However, over the past decade, new financial accounting rules have forced states and districts to start recognizing and publicly reporting those costs, which is likely to put even more downward pressure on teacher salaries and other school spending. These trends are contributing to broader teacher unrest, and were factors in recent teacher walkouts in states like Colorado, Kentucky, Oklahoma, and West Virginia.
The escalating costs are poised to raise the profile of these post-employment health benefits. And the ensuing debate is sure to raise broader questions about what districts owe their retirees and whether they can make good on the promises as written, or if there are reforms that could balance worker protections with responsible budgetary practices. Moreover, the problem with retirees’ health benefits extends beyond their cost or divergence from the private sector; there are also reasons to doubt whether these benefits help schools attract and retain high-quality workers. In this piece, I review the history and landscape of retiree health benefits, explain why those plans might not be having the desired effects on the teacher workforce, and explore options for reform.
Reckoning with retirement costs
The first retiree health-benefit plans started out in the 1940s as a way to attract and retain workers in both the private and public sectors, which competed with each other and offered similar health benefits. For decades, employers were able to offer retiree health benefits as part of employees’ compensation packages without fully accounting for their cost.
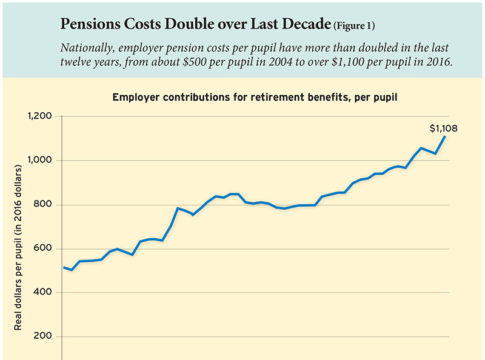
That began to change in the private sector in the mid-1980s, when new accounting rules forced companies to include the long-term liabilities of post-employment health-care benefits on their balance sheets. As workers aged into the plans and began collecting benefits, companies were required to properly account for the projected expense of future promises and make those liabilities public, rather than just reporting the annual costs of paying for the benefits that year. Companies quickly decided it made more sense to close the plans than to appear less profitable. The share of large and midsize companies offering retiree health benefits fell from 45 percent in 1988 to 24 percent in 2017, Bureau of Labor Statistics data show (see Figure 1). Smaller companies are even less likely to offer such benefits, and nationally, just 15 percent of private-sector workers have access to employer-provided retiree health benefits.

For public-sector workers like teachers, the numbers remain much higher. In 2017, 69 percent of public-school teachers were employed in states or districts that offer retiree health benefits to workers under age 65, and 61 percent of teachers worked for an employer that offers health benefits even after age 65, when all Americans become eligible for Medicare. However, a similar change in accounting rules for state and local agencies was adopted in 2008, forcing states and local governments to publicly report long-term obligations they had long ignored. The question is, what will states and districts do in response?
We may find clues based on the size of the liabilities. As a point of comparison, readers may be familiar with unfunded pension liabilities in the public sector. As of 2016, the gap between state pension systems’ funds and obligations had grown to $1.4 trillion nationwide, including about $500 billion for education workers. But those figures do not include the cost of retiree health care, and while we don’t have the data needed to determine a firm estimate, we can get a sense of the scope of the financial challenges ahead. According to the Pew Charitable Trusts, 35 states offer former public employees health benefits in retirement, and they’ve accumulated a total unfunded liability of $692 billion. Roughly one third of all public employees in the United States are teachers and other education workers, so it’s reasonable to estimate that unfunded health-care promises amount to about one third of the total liability, or about $231 billion just for teachers and other public-education employees. Some school districts, like LAUSD, offer their own benefits as well, either on top of the state plan or in lieu of one.
Precarious plans
While the unfunded promises for retiree health care are only half as large as they are for pensions in terms of total dollar amounts, the health benefits are in much worse shape in terms of the money states have saved for the future. Nationwide, public-sector pension plans are 65 percent funded, meaning that states have saved 65 cents for every dollar promised in future benefits. This is not good, and it’s the main reason pension contributions have skyrocketed in recent years, putting pressure on state budgets.
Health care for retirees is on even shakier ground. Until recent years, states were not required to calculate how much retirees’ health-care promises were worth, and few put anything aside to pay for them in the future. Today, 15 states, including large ones like Florida, New Jersey, and New York, have zero dollars set aside to pay for retiree health-care obligations. Nationwide, future projected health-care costs for retirees are 7 percent funded, with other large states posting even lower ratios: California has a funded ratio of 0.2 percent, Connecticut is at 1.0, Pennsylvania at 1.6, and Texas is at 1.2 percent (see Figure 2). Put simply, there is no money saved to cover 93 percent of the anticipated costs for retirees’ health-care benefits.

That may make these benefits especially vulnerable to budget pressure. Unlike pensions, which are covered by legal provisions that restrict the changes that states can make for existing workers and retirees, retiree health benefits have no such protections. They could be on any budget chopping block at any time. Pensions may be where the bulk of the long-term costs pressures are, but policymakers may prefer reforming retiree health benefits for the more immediate cost savings.
These factors create a precarious situation, and the most obvious solutions are to adopt steep benefit cuts or increase contributions. States and districts have been busy in recent years restricting eligibility only to very long-term employees, and it’s likely this trend will accelerate. If states also step up required contributions, that will lower take-home pay for all teachers. Combined, these two trends would require all teachers to pay for a benefit few of them will qualify for once they reach retirement age.
Rather than going down this path, state leaders should figure out compromise solutions now that will balance rising cost pressures with protections for workers. But before turning to potential solutions, it’s also worth considering how the plans affect teacher decisions around retention and retirement.
Limited role in retention
Although retiree health benefits have historically been justified on the grounds of boosting teacher recruitment and retention, there are reasons to doubt how effective they are at accomplishing those goals. To my knowledge, there have been no studies examining whether post-employment health-care benefits affect the recruitment or early-career retention of teachers. But the research base on pensions is illustrative. In a recent paper, Matthew Kraft, Eric Brunner, Shaun Dougherty, and David Schwegman did not find any evidence that increases in employee contribution rates toward pension plans harmed teacher recruitment efforts. That is, incoming teachers either didn’t know about the cost increases, or the increases weren’t sufficient to change teacher behavior.
My hunch is that new teachers are similarly unaware of how retiree health benefits work. When my colleague Kelly Robson and I looked at state pension-plan assumptions on teacher turnover, we found no state that assumes its early-career teachers will change their behavior in order to qualify for a pension benefit (see “Why Most Teachers Get a Bad Deal on Pensions” at www.educationnext.org). Other studies, such as one looking at a large benefit change to the pension plan in the St. Louis Public Schools, have found that pension plans can help retain late-career workers. However, only a small fraction of teachers remain on the job for that long, and after they reach the maximum years of service and benefit level, pension plans effectively push them into early retirement.
Retiree health-care plans are likely to have similar null effects on teacher recruitment and retention, especially at the front end of teachers’ careers. What about at the back end? A study by Maria D. Fitzpatrick found that the guarantee of post-employment health-care benefits helped push out older teachers in Illinois. She concluded, “The median older worker in [Illinois Public Schools] retires two years earlier than they otherwise would have because of the availability of retiree health insurance.” In other words, retiree health plans push experienced, veteran teachers and principals out of schools and districts and into retirement.
If the plans have not historically boosted teacher retention, they’ll do an even worse job of that going forward. That’s because states and local governments are responding to cost pressures by limiting who is eligible for benefits. For example, in years past, New York City offered city workers health benefits in retirement if they had five or more years of service. But that term was changed to 10 years for workers hired after 2000, and 15 years for workers hired after 2009. LAUSD has seven different tiers of retiree health benefits, depending on when the employee entered the district and when he or she retires. Each tier is more restrictive than the one that came before it, and the minimum service requirement has shot up from 5 to 25 years for full-time employees hired after 2009. In these cities, fewer and fewer workers will qualify for retiree health benefits, even as the city is paying higher and higher shares of its budget toward the program.
States have enacted similarly restrictive policies on who is eligible for retiree health benefits, with the result that only long-term veterans will qualify. A review of state pension-plan assumptions shows just how small this group is projected to be. For example, New Jersey offers teachers who serve for at least 25 years post-employment health-care benefits, but according to the state pension-plan’s assumptions on teacher turnover, most teachers won’t make it that far. Similarly, a young teacher in Texas would have to serve for 30 years before qualifying for the state’s post-employment health-care benefit, but the state’s pension projections estimate that only one in five new teachers will qualify. Meanwhile, all Texas teachers have to pay 0.65 percent of their own salaries toward retiree health-care benefits, their district employers contribute another 0.75 percent, and the state chips in 1.25 percent.
These plans are costing all teachers money, but they are becoming so limited that they reach only a small fraction of the workforce. That puts states in an uncomfortable position. States are implicitly acknowledging that the plans won’t act as a retention incentive for the majority of workers while they preserve extra benefits for workers with the most stable work histories. As the plans’ costs rise, they have become even less of a retention incentive and less of a protection to workers who might truly need the coverage.
A potential federal fix
Even if current retiree health-benefit plans are not an effective tool to shape the teacher workforce, policymakers might still want to ensure that former teachers in their 50s and 60s have access to health care. There is a range of options for policymakers looking to balance rising costs with the desire to provide adequate health benefits to a vulnerable group of retirees.
At one end, employers could just buck up and make the necessary payments. Or, they could keep the basic benefit structures intact and impose stricter limits on who is eligible to receive retiree health benefits. This approach might be preferable to current beneficiaries, but it follows an unsustainable trajectory. At some point, a generation of teachers is likely to balk at paying for a benefit that is no longer available to them, or available only to a few long-serving members of their cohort. Taxpayers might also balk at spending more on education and seeing a smaller and smaller portion of their investment actually make it into classrooms.
At the other end of the spectrum, some policymakers might be tempted to end their programs altogether. North Carolina, for example, recently announced it would not offer retiree health benefits to state workers who begin their employment after January 2021. (This does not affect teachers, who are enrolled in a separate plan.) Other states may be tempted to follow suit. Why, after all, should public-sector workers be given a benefit that most private-sector workers don’t have? And why should the public offer a benefit that systematically encourages employees to retire at relatively young ages?
The North Carolina model may sound draconian at first, but it’s worth a second look, mainly due to Obamacare. The federal Affordable Care Act provides subsidies on a sliding scale to individuals to purchase health insurance, regardless of age; in 2018, a two-member household earning less than $65,840, or 400 percent of the federal poverty level, would qualify for assistance. That’s more than the average and even the median teacher pension in most states as of 2016 (the most recent year with data available). Assuming no other sources of income, many former teachers could qualify for federal subsidies that would cover at least some costs of a health-care plan.
This move would effectively shift retiree health-care liabilities to federal taxpayers, but it might ultimately be more efficient to tie benefits to income and need rather than years of service. Moving former state and local government employees onto the Obamacare exchanges could also help stabilize private insurance markets by providing a new source of enrollees.
Similarly, the Obamacare exchanges are designed to be a bridge to Medicare, but many states and districts still provide benefits beyond that point. It seems reasonable to limit future benefits to retirees under age 65, who have not yet qualified for Medicare. Medicare offers a reasonable floor of benefits open to all, and there’s little public purpose accomplished by subsidizing benefits beyond that. Instead, employers could sponsor health savings accounts for workers who have the means and want to save on their own for additional medical expenses on top of Medicare.
Other than federal taxpayers, the main losers from this arrangement would be medium- and higher-income retirees who currently qualify for retiree health benefits. States could choose to offer additional contributions for those workers who wouldn’t qualify for federal subsidies because their pensions were too large or because they had other sources of income. But this would not be the best use of limited resources. Ultimately, policymakers should question whether it’s a good public investment to pay for the health care of former workers who already have generous incomes, either from their government pensions or other sources.
For places that don’t have Obamacare exchanges or don’t want to use them for this purpose, state and district leaders should still try to focus their resources on those who need it most. This differs from the current path, in which states and districts are looking to restrict eligibility for the same benefits rather than changing the underlying benefit itself. Instead, they could shift their coverage offerings from comprehensive “Cadillac” plans to more modest “catastrophic” plans, which could be extended further to protect more families from unexpectedly high health-care burdens.
Lessons at the state level
There are 35 states that offer post-employment health coverage to teachers, following three basic models: providing access to group plans at the retiree’s expense, covering a fixed percentage of retiree health-care costs, or contributing a fixed dollar amount toward the costs.
In the first model, states and districts play the role of health care provider rather than health care payer. Five states do this, providing retirees access to health insurance plans but no employer contribution toward those benefits. In these states, retirees can purchase a dedicated health-insurance plan and get the benefit of group pricing, but they must pay their own premiums.
This model looks similar to other policies that already exist to protect individuals who are out of work. Through the federal continuation health-coverage program, COBRA, the U.S. government requires employers to grant former employees access to their same health-care plan for up to 18 months post-employment, so long as the former employees pay the full cost of monthly premiums and administrative fees out of pocket. Many employees already use COBRA as a bridge from employment to Medicare, and states could simply extend COBRA coverage for former state and local government employees until they reach age 65. There would be minimal costs to a state that pursued this route—again, they would not be paying for any retiree’s health care—and though COBRA may be an expensive option for retirees, it would at least give them high-quality options beyond the private market.
For states that don’t want to rethink their coverage provisions, they should at least rethink their payment options. They may be forced to do so anyway. Some 23 states contribute a fixed percentage of retirees’ health-care costs each year, which shields employees from the full costs of the plans and leaves the state on the hook to keep up with the bulk of any increases. Teachers might see their own costs go up as well, but they rarely see what their state or employer is contributing. The states that have chosen to make fixed-percentage payments have accrued higher liabilities than those that contribute a fixed-dollar amount, and the only immediate recourse is to shift a larger percentage of the costs onto current workers (see Figure 3). That is already happening in some places—the recent teacher walkout in West Virginia was largely driven by this scenario—and similar budget pressures may encourage other states to follow suit.

Another option would be to follow the seven states that contribute based on a fixed-dollar amount, which effectively caps the state’s future liabilities. Much like the shift in retirement toward defined-contribution plans, this move would place a higher burden on retirees. But it could potentially help control broader health-care costs over the long term if the end user, workers, have more financial stake in their own health care. At the very least, it could give workers a greater appreciation for how much their health care actually costs and create demand for broader cost reductions.
The latest actuarial report from Los Angeles highlights the urgency of putting one of these strategies in place. LAUSD is projected to make retiree health-benefit payments totaling $306 million this year. Those numbers are projected to double in the next nine years. With a current enrollment of 620,000 students and 25,000 teachers, that means the district already is spending about $493 per pupil and $12,221 per teacher to provide former employees, their spouses, and dependents with free medical, dental, and vision coverage. As the district faces a potential teacher strike this fall, these costs—and the unfunded promises that created them—loom large in the background.
None of the options presented here will be politically popular, but cost pressures will increasingly force states and local school districts to think differently about retiree health benefits. For too long, employers were able to promote the benefits without recognizing their long-term costs. That reckoning is coming, and there are better and worse ways to tackle it.
Chad Aldeman is a principal at Bellwether Education Partners and the editor of TeacherPensions.org.
This article appeared in the Winter 2019 issue of Education Next. Suggested citation format:
Aldeman, C. (2019). Health Care For Life: Will teachers’ post-retirement benefits break the bank? Education Next, 19(1), 28-35.